
RACGP KFP 2017.2 Case 13: Bob is a 76 year old man who presents to your remote rural practice with 2 days of progressing shortness of breath on mild exertion. His part history includes Hypertension, COPD, previous angina, DVT, BPH, Cirrhosis, Aortic Stenosis. His medications include duodart, perindopril 10mg, and symbicort 200/6 bd.
What are the most important differentials in this patient to consider? (List 5)
- Acute Myocardial infarction
- COPD infective exacerbation
- Arrhythmia
- Pulmonary Embolism
- Exacerbation of Congestive Cardiac Failure – fluid overload
Others:
- Decompensated aortic stenosis
- Secondary pneumothorax
- Anaemia (less likely give short history but possible if marked bleed e.g. intraabdominal)
What are the most important initial investigations to order? (List 8)
- ECG
- Chest Xray
- Troponin
- ABG
- D-dimer – DVT/PE
- FBE – anaemia
- EUC – for arryhthmia
- CRP – infection
Others:
- Holter
- Echo – unlikely to be initial
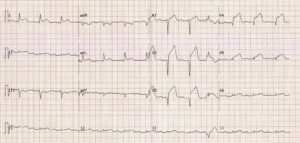
During the consult, the patient complains of chest pain, central chest, 9/10 which he describes as crushing, associated with an increase in his shortness of breath.
Examination shows:
Obs: T 36.6, PR 110 reg, BP 110/70, RR 20, O2 96% RA, GCS 15
Respiratory examination: normal apart from findings above
Cardiovascular examination: normal apart from findings above, nil calf swelling
ECG:
What are the most important initial management steps to undertake (List 5)
- Call Ambulance
- IV Access
- aspirin 300 mg chewed or dissolved before swallowing.
- glyceryl trinitrate spray 400 micrograms sublingually, repeat every 5 minutes if pain persists, up to a maximum of 1200 micrograms
- morphine 2.5 to 5 mg IV, as an initial dose, then titrate to effect every 5 to 10 minutes with further incremental doses of 2.5 to 5 mg.
Giving oxygen would give no marks. “In patients with suspected or proven acute coronary syndromes and the absence of hypoxia, the benefit of oxygen therapy is uncertain, and in some cases oxygen therapy may be harmful. It is recommended that oxygen administration be targeted to achieve oxygen saturation(SpO2) of 94-98%.” https://www.nzrc.org.nz/assets/Guidelines/Adult-ALS/ANZCOR-Guideline-11.6.1-Targeted-Oxygen-Therapy-Jan2.pdf
References:
https://www.nzrc.org.nz/assets/Guidelines/Adult-ALS/ANZCOR-Guideline-11.6.1-Targeted-Oxygen-Therapy-Jan2.pdf
(1) NICE (May 2007). Secondary prevention in primary and secondary care for patients following a myocardial infarction
(2) NICE (March 2010). Assessment and diagnosis of recent onset chest pain or discomfort of suspected cardiac origin – https://www.nice.org.uk/guidance/cg95/chapter/Recommendations
(3) NICE (July 2013). Myocardial infarction with STsegment elevation – The acute management of myocardial infarction with ST-segment elevation
https://emedicine.medscape.com/article/155919-treatment#d5
MJA article (2013) – The approach to patients with possible cardiac chest pain
RACGP Feedback – Case 13
This case featured an older male adult with a previous history of chest pain who now has acute shortness of breath that developed over the preceding two days. The patient’s full medical history, including medications, is provided.
Candidates needed to identify the differential diagnoses and investigation and, as the case unfolds, the immediate management of acute chest pain in the general practice environment. The most common errors seen in this question were providing a list of all causes of shortness of breath and not focusing on the information provided, as well as providing non-specific answers.
When considering which investigations to include, it is important to read the question; in this case, initial investigations were required to address the causes for the acute shortness of breath, not ongoing outpatient investigations such as stress echocardiography.
Candidates need to consider which investigations will give the best return on information to assist in diagnosis, rather than selecting what are often seen as ‘baseline’ investigations. In managing acute chest pain in the practice setting, candidates need to be aware of current guidelines, including those regarding the use of oxygen. The case required specific management steps, with candidates expected to provide appropriate drug regimens rather than just listing drug names.
RACGP Conclusion on Technique
As outlined above, there are some common themes and key issues to consider when approaching the KFP exam:
- The KFP exam is not a simple short-answer paper. You must answer the question in the context of the clinical scenario provided, utilising all of the information provided. Read the scenario at least twice.
- Keep your answers succinct.
- Only provide the number of answers requested. Review your answer – have you created a list rather than one answer per line? If so, you will be penalised for extra answers.
- Always read the question at least twice and, after you answer, check that you have answered the actual question asked.
- Be specific in your answers, whether in the investigations being ordered or the treatment you are prescribing. Non-specific answers will not score or will attract a much lower score.
- General answers such as ‘educate’, ‘refer’, ‘reassure’ or ‘review’ do not score without specific detail. For example, providing a review timeline and details about the specialist to whom you are referring (along with degree if urgency, if appropriate) may score marks if relevant to the scenario and question.
- Be aware of clinical guidelines and any important changes or additions to treatments. If guidelines change very close to the exam, the marking keys are adapted to consider the original and the new guidelines so candidates are not penalised if they have not seen a guide published close to the exam sitting.
- Access the practice exams provided after enrolment closes and utilise the RACGP assessment resources provided for candidates.





